Overtraining, Autoregulation, and Your Sex Life
Prior to discussing the relationship between heart rate variability, over training, and sex drive, we must first revisit the basic anatomy and physiology of the nervous system. The nervous system is divided into two components, the central nervous system and the peripheral nervous system. While the CNS is comprised of the brain and spinal cord, the PNS is divided between the autonomic (ANS) and sensory-somatic nervous system. For the purpose of this article, it is the autonomic nervous system we are concerned with.
The ANS is responsible for the control of the internal environment, including respiration, circulation, digestion, immunity, etc. The ANS is further divided into two antagonist branches: the sympathetic (SNS) and parasympathetic (PNS) nervous systems. SNS tone is increased to raise heart rate, systolic blood pressure, adrenal secretions, and diverting blood flow to the muscles. In contrast, the PNS reduces heart rate, systolic blood pressure, and increases blood flow to the gut.
In the context of this article, training activates the SNS while rest should increase PNS tone, and collectively they work in harmony to maintain a homeostatic internal state. In the overtraining syndrome the contributions of SNS:PNS tone is altered, such that either: A. SNS activity is increased at rest and submaximal work; B. PNS activity does not increase with rest; or, C. inability of SNS activity to increase heart rate during exercise (Fry et al., 2006). Therefore, if we can monitor ANS activity, we can more easily autoregulate and prevent overtraining. Enter heart rate variability (HRV).
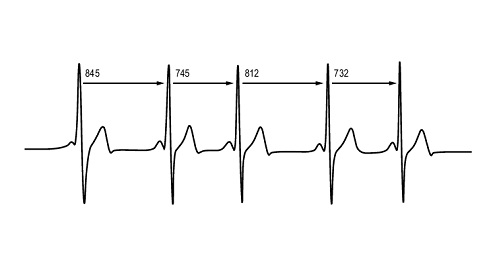
Heart rate variability is the alteration in interbeat intervals without an appreciable change in heart rate (Taylor & Lipsitz, 1997). In essence, if the heart rate is 60 BPM and there is exactly 1 second between the initiations of each beat, then HRV is 0. On the other hand, if the heart rate remains at 60 BPM but there is a range of .66 to 1.3 seconds between consecutive beats, then HRV exists. The easiest way to display this concept is by measuring the distance (or time) between heart beats on an EKG readout, as seen below:
We can then calculate the mean, summate and average the variations in distances between heart beats over a period of time, and take their square root to calculate HRV (Taylor & Lipsitz, 1997):

A simple way to demonstrate the concept of HRV is by imagining the effect that breathing has on heart rate. Inspiration increases SNS activity and thereby every time you take a breath in, your heart rate increases. In contrast, expiration increases PNS activity, and when you breathe out heart rate decreases. This relationship between respiration, heart rate, and ANS activity is displayed below.

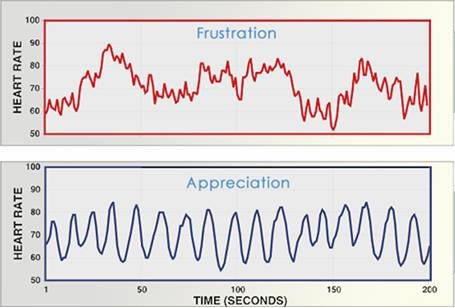
Physical and emotional challenges place a stress upon the organism to maintain homeostasis. The stress associated with the commencement of a new training regimen is sensed by the organism and met with an increase in SNS tone. As a result, the pituitary signals the secretion of adrenal stress hormones (cortisol, epinephrine) and HRV starts to decrease. The HRV response to acute stress is illustrated below: note the difference in frequencies between appreciation (relaxed) and frustration (stressed).
If training is continued without adequate adaptation then a plateau in gains will occur and eventually performance will start to decrease. This plateau in performance is accompanied by beta-adrenergic receptor down regulation (Fry et al., 2006) and manifests in the additional time required to elevate the heart rate during a warm up. As a consequence of down regulation, SNS tone is increased further and adrenal stress hormones remain elevated thus inhibiting protein synthesis (repair) and leading to the decrease in performance (Angeli et al., 2004). 24 hours following exercise PNS tone is increased to a greater magnitude, and thus HRV increases during these periods of non-functional overreaching (Thayer & Sternburg, 2006).
If adaptation fails and training continues overtraining ensues. Overtraining is seen in the neuroendocrine system as impaired SNS activation and bodily response (also commonly known as adrenal fatigue). It manifests in elevated resting cortisol, elevated diurnal cortisol, elevated resting heart rate, significantly increased or decreased HRV, inability to recover from exercise, and susceptibility to illness (Angeli et al., 2004).
On the other hand, if ANS activity is monitored, over-reaching is identified, and a period of unloading or reduced stress follows then supraphysiological adaptations will occur (which many experience as improved strength following a week of complete rest). The below diagram illustrates the model of stress, adaptation, overtraining, and supracompensation. Ideally, we wish to cease intense training where the dip in performance begins (red circle) in order to avoid exhaustion (overtraining) and initiate supracompensation adaptations.

The diagram below illustrates the different processes occurring as the individual goes from training, to over-reaching (high activation), non-functional over-reaching (over-activation), and then overtraining syndrome (stress). Seen below is that during the period of high activation anabolic processes (recovery and building), metabolic processes (ability to generate energy), and workability state (performance) are nearly maxed out, while catabolic processes remain relatively low. This state would refer to the first significant increase in HRV and be marked by the plateau in performance. Over activation marks the stage where performance (in this case strength) starts to decrease and HRV continues to rise above baseline. Over activation also corresponds to the dip in performance marked by the red circle above. Moving further to the right is overtraining, whereby catabolic processes far outweigh anabolic processes and performance is significantly reduced.

HRV may provide us with a simple, non-invasive method in which to either auto-regulate daily training volumes and intensities or identify the start of over-reaching prior to the appreciable reduction in performance. In a case study of two athletes, Plews et al. (2012) reported a link between reduced HRV, non-functional over-reaching, shingles reoccurrence, and poor triathlon performance. Chen et al. (2011) reported a relationship between HRV, DHEA, muscle damage, and performance following an acute weight lifting session. In particular, 3 hours after training HRV, muscle damage and performance were reduced. Following 48 hours, DHEA levels returned to baseline while HRV and performance both increased. The results indicate that PNS induced elevations in HRV frequency following acute training may reflect the recovery status of the athlete.
Too much PNS activation, however, is also indicative of impaired recovery. Tian et al. (2012) investigated the differences in HRV between functional over-reaching and non-functional over-reaching (intense training with recovery) in elite women wrestlers training for 11 competitions over the course of 2 weeks. Subjects who responded normally to training displayed a HRV of 82.8 ms while subjects who did not respond to training displayed either a reduced HRV of 46 ms or a hyper-responsive HRV of 160.4 ms. Therefore, monitoring severe perturbations in HRV both above and below baseline that last in excess of 2 weeks can be used identify the transition to non-functional over-reaching and may be a useful tool in precisely programming unloading periods following intense training.
There are a number of smart phone applications available to monitor HRV with the use of a heart rate monitor that will even advise you to train hard or not that specific day. Some of these are mentioned in a similar article at T-Nation regarding HRV training. As discussed by Pope and Weller, there are some limitations to these, including the inability of the application to determine whether the change in HRV is due to emotional stress or training (both of which feed into overtraining syndrome).
Rather than comparing to baseline HRV values as suggested by Pope and Weller, a more accurate measure to compare may be HRV recovery values. The first step in doing so is similar to comparing to baseline values in that one must unload for a week to get an accurate HRV reading. Then, have the athlete perform a simple, low intensity progressive bike test. The internal rate of the heart is about 100 beats per minute (Levy & Pappano, 2007) and represents how fast a healthy heart would beat without the SNS or PNS acting upon it.
Our goal is to slowly elevate this to where just a little SNS tone is present, or approximately 110-115 beats per minute, maintain for 6 min, and measure HRV at the end of exercise. This value will represent the upper end of the HRV spectrum. Then immediately stop pedaling. At this point the PNS will kick in and start to decelerate the heart. After 2 min and every 2 min thereafter measure heart rate and HRV a total of 10 min. Record your highest HRV (the upper end of the spectrum) and the change in between exercise and 2 min of recovery (Procedures schematic shown below).

We now have both an HRV spectrum and an HRV recovery value to compare to. Both will allow you to monitor ANS function. Measure HRV at the same time each day and compare these values to the spectrum. Over the course of a few weeks after starting a new training program you should observe a normal decrease and then rise in HRV associated with stress and response, respectively. If that rise or fall in HRV is outside of the spectrum, and recovery HRV (measured via the same bike test) is also impaired, then it is likely the athlete is close to transitioning into the state of non-functional over-reaching and a week of reduced intensity and/or volume (unloading) is required.
Most readers are now wondering: what does all this have to do with sex drive? First, let us mention that disruptions in HRV, specifically lower resting HRV, are associated with negative clinical outcomes such as inflammation, impaired glucose regulation, excess visceral fat, and elevated low-density lipoprotein cholesterol, as well as all-cause mortality (Thayer & Lane, 2007). Now then onto more juicy information. Costa and Brody (2012) performed an interesting study to determine if there was a correlation between HRV and intercourse frequency. Because PNS tone is important for sex organ function; impaired HRV (due to increased resting SNS activity) is associated with erectile dysfunction; and, sensory information from the vaginal nerves are relayed to the brain via vagal (PNS) afferent nerves, Costa and Brody hypothesized that greater HRV would be associated with greater sexual intercourse and female orgasm, and vice versa.
The results reported by Costa and Brody support their hypothesis: greater HRV was correlated with more frequent intercourse for both men and women, and more frequent orgasms in women. As we have seen earlier, non-functional over-reaching is associated with increased SNS activity, reduced PNS activity, and also anecdotal reports of a decline in libido. Taken collectively, HRV can be used to not only autoregulate and improve performance, but also ensure that stressors associated with training do not reduce libido or disrupt sex life.
References:
Angeli, A., Minetto, M., Dovio, A., & Paccotti, P. (2004). The overtraining syndrome in athletes: a stress-related disorder. Journal of endocrinological investigation, 27(6), 603–12. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/15717662
Chen, J.-L., Yeh, D.-P., Lee, J.-P., Chen, C.-Y., Huang, C.-Y., Lee, S.-D., Chen, C.-C., et al. (2011). Parasympathetic nervous activity mirrors recovery status in weightlifting performance after training. Journal of strength and conditioning research / National Strength & Conditioning Association, 25(6), 1546–52. doi:10.1519/JSC.0b013e3181da7858
Costa, R. M., & Brody, S. (2012). Greater resting heart rate variability is associated with orgasms through penile-vaginal intercourse, but not with orgasms from other sources. The journal of sexual medicine, 9(1), 188–97. doi:10.1111/j.1743-6109.2011.02541.x
Fry, A. C., Schilling, B. K., Weiss, L. W., & Chiu, L. Z. F. (2006). beta2-Adrenergic receptor downregulation and performance decrements during high-intensity resistance exercise overtraining. Journal of applied physiology (Bethesda, Md. : 1985), 101(6), 1664–72. doi:10.1152/japplphysiol.01599.2005
Levy, M., & Pappano, A. (2007). Cardiovascular Physiology (9th ed.). Mosby.
Plews, D. J., Laursen, P. B., Kilding, A. E., & Buchheit, M. (2012). Heart rate variability in elite triathletes, is variation in variability the key to effective training? A case comparison. European journal of applied physiology, 112(11), 3729–41. doi:10.1007/s00421-012-2354-4
Taylor, J. A., & Lipsitz, L. A. (1997). Heart rate variability standards. Circulation, 95(1), 280–1. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/8994452
Thayer, J. F., & Lane, R. D. (2007). The role of vagal function in the risk for cardiovascular disease and mortality. Biological psychology, 74(2), 224–42. doi:10.1016/j.biopsycho.2005.11.013
Thayer, J. F., & Sternberg, E. (2006). Beyond heart rate variability: vagal regulation of allostatic systems. Annals of the New York Academy of Sciences, 1088, 361–72. doi:10.1196/annals.1366.014
Tian, Y., He, Z.-H., Zhao, J.-X., Tao, D.-L., Xu, K.-Y., C P Earnest, & Mc Naughton, L. R. (2012). Heart rate variability threshold values for early-warning non-functional overreaching in elite women wrestlers. Journal of strength and conditioning research / National Strength & Conditioning Association, Epub Ahead of Print. doi:10.1519/JSC.0b013e31826caef8

Spot on with this write-up, I really feel this web site needs a grezt deal more attention.
I’ll probably be back again to read through more, thanks for the advice!